Osimertinib, a third generation EGFR-TKI, is the standard of care in first-line treatment of patients with EGFR-mutated non-small cell lung cancer (NSCLC). Upon disease progression, platinum-based chemotherapy has been one of the usual approaches. A recent analysis of the global COMPEL trial suggests that continuing osimertinib with combination platinum and pemetrexed is superior to chemotherapy alone in patients whose disease has progressed on first-line osimertinib in the absence of intracranial progression.
“Progression on first-line osimertinib is sometimes heterogeneous, with some cells—especially within the central nervous system (CNS)—retaining EGFR signal independence and sensitivity to EGFR tyrosine kinase inhibition,” said Giulia Pasello, MD, PhD, Associate Professor of Oncology at the University of Padova and Veneto Institute of Oncology in Padova, Italy. “Osimertinib may continue to exert a protective effect in the CNS following progression.”
Dr. Pasello presented results from the COMPEL trial during an oral abstract session titled Improving Outcomes in EGFR and KRAS Mutant Tumours, More is Better? on Monday afternoon at the 2025 World Conference on Lung Cancer.
Due to changes in the treatment landscape, the trial ended early with 98 patients randomized. Patients were stratified by the presence or absence of CNS metastases. About a third of patients had brain metastases at baseline; on average patients had received osimertinib for about 20 months before entering the trial.
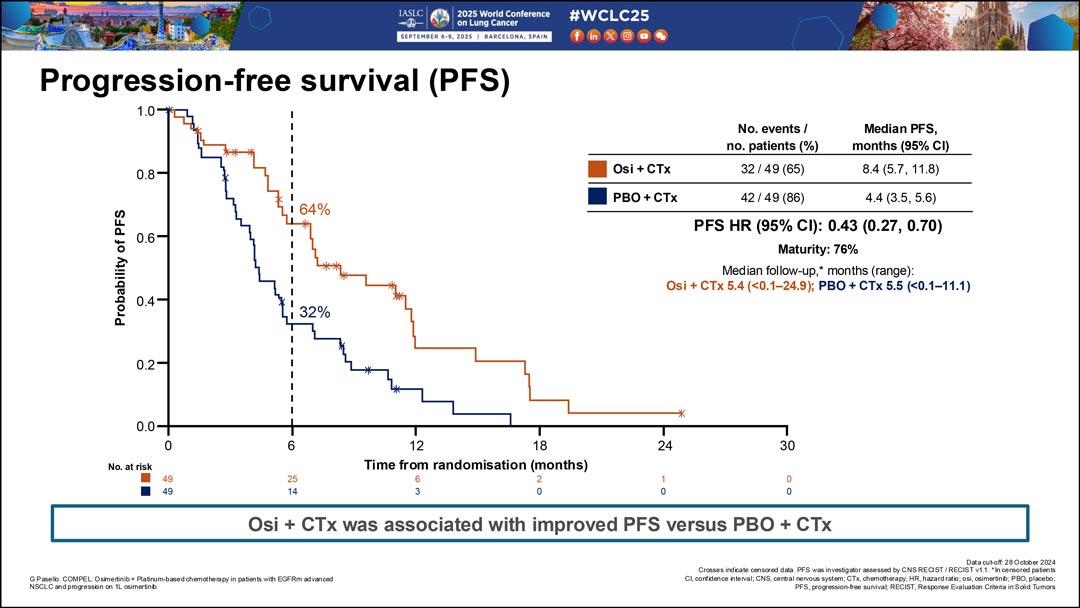
The study was underpowered to statistically assess the primary endpoint of investigator-assessed progression-free survival (PFS), however combination therapy yielded a median PFS of 8.4 months compared to chemotherapy alone (4.4 months).
When assessed by CNS metastases at baseline, patients without baseline CNS tumors on combination therapy had a 6-month PFS of 87% compared to 63% for patients on chemotherapy plus placebo [hazard ratio (HR) 0.56 (95% confidence interval [CI] 0.27 – 1.13)]. The median CNS PFS was 15.9 months for the combination arm compared with 8.6 months for the placebo arm.
Additionally, Dr. Pasello said patients on the combination therapyhad fewer new lesions (18% vs. 25%) and fewer new brain lesions (5% vs. 13%). She said that at the time of progression, 10% of patients with disease progression on combination therapy had developed new brain lesions compared with 27% of patients on chemotherapy plus placebo.
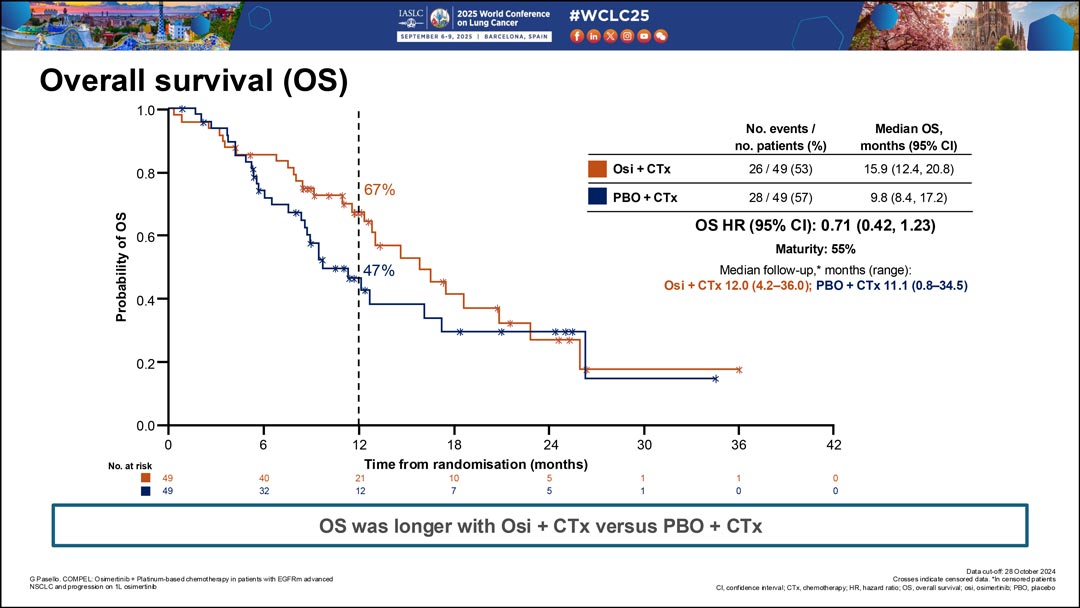
Overall survival (OS) at 12 months was 67% for the combination therapy and 47% for chemotherapy plus placebo [HR 0.71 (94% CI 0.42 – 1.23) at 55% data maturity. Median OS was 15.9 months for the combination therapy and 9.8 months for chemotherapy plus placebo.
The data showed no new safety signals, and adverse events (AEs) were consistent with the known safety profiles for the combination of osimertinib with platinum and pemetrexed. Unfortunately, because of limited overall accrual, the study—despite apparent improvements in PFS, OS and intracranial progression—was underpowered to demonstrate statistical significance.