






A secondary analysis of the randomized clinical trial Cancer and Leukemia Group B (CALGB) 140503 investigated oncologic outcomes in patients with non-small cell lung cancer (NSCLC) who had visceral pleural invasion (VPI) following lobar or sublobar resection.1
Ramón Rami-Porta, MD, PhD, Clinical Chief of the Department of Thoracic Surgery at Hospital Universitari Mútua Terrassa, in Terrassa, Barcelona, Spain, provides expert insight and a surgical perspective on the implications of the recent analysis.






Surgical Implications of the Secondary Analysis
The analysis of the T2 tumor subgroup showed no difference in disease-free survival (DFS) between patients who had lobectomy and segmentectomy, suggesting that both lobar and sublobar resection are equal.

It is important to keep in mind that these T2 tumors were so classified by virtue of their VPI, not by their tumor size. The tumors included in this clinical trial were 2 cm or less in greatest dimension (clinical T1a and T1b by the 9th edition tumor, node, and metastases [TNM] classification) and had no nodal involvement at clinical evaluation. According to the definitions of the TNM classification, these small tumors with VPI are classified as T2 and not as T1, which would be their T category based exclusively on tumor size.
All that said, the surgical implication of the trial is that patients with peripheral tumors of 2 cm or less in size can undergo either segmentectomy or wedge resection (wedges were allowed in this North American trial), because their outcomes are not inferior to those of lobectomy. However, one must consider that the long-term follow-up of the Japanese trial on the same topic—but with important differences, such as inclusion and exclusion criteria, intraoperative nodal evaluation, etc.—confirmed what it showed at the time of initial publication: that segmentectomy (wedges were not allowed in this trial) was associated with higher rates of recurrences, even if DFS and overall survival (OS) were the same for segmentectomy and lobectomy.
Even if it does not have an impact upon OS, a recurrence can have a major impact on patients. Recurrence is a shock for patients, relatives, and managing physicians. It implies an indication for new diagnostic and staging procedures, and new therapies that, maybe, a lobectomy would have spared. So, in my opinion, segmentectomy and wedge resection should be indicated with caution in patients who can otherwise undergo lobectomy.
Challenges to Traditional Clinical Assumptions on Recurrence Risk in Small Tumors
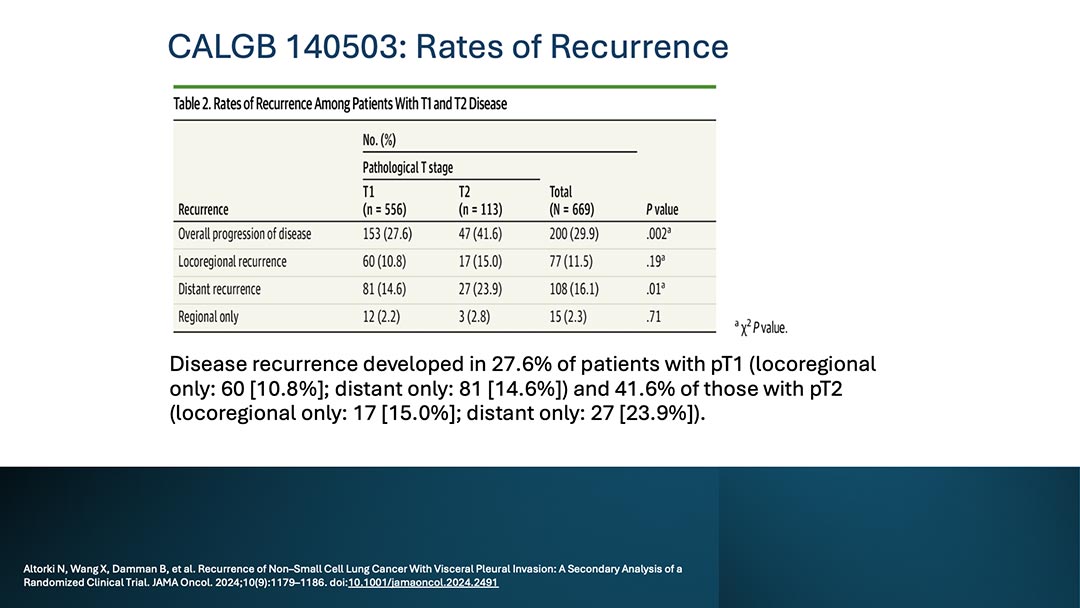
The study found that patients with small (≤ 2 cm) peripheral NSCLC with VPI (pT2) had unexpectedly higher recurrence rates and poorer survival compared to patients with tumors without VPI, regardless of the surgical technique used.
In my opinion, these findings do not present any challenges. Since the publication of the 2nd edition of the Union for International Cancer Control TNM Classification of Malignant Tumours and the 1st edition of the American Joint Committee on Cancer Cancer Staging Manual, published in 1968 and 1977, respectively, VPI has been a T2 descriptor, and T1 tumors with VPI have been classified as T2 because they really have a T2 prognosis.
The worse prognosis of VPI has been confirmed in more recent studies, and VPI even has two categories depending on the depth of its invasion: the invasion of the elastic layer of the visceral pleura but not the lung surface, and the invasion of the lung surface, which has a worse prognosis than the mere invasion of the elastic layer. The VPI facilitates tumor spread along the subpleural lymphatic network and, therefore, it is not surprising that these tumors are frequently associated with nodal involvement and recurrence.
High Recurrence Rates Independent of Surgical Technique and the Implications for Adjuvant Therapy
The study leaders suggest that the data reported above support including these patients in adjuvant therapy trials.
This is an interesting finding: a larger resection does not counteract the deleterious effect of VPI. VPI is associated with increased cancer recurrence, whether the resection has been a lobectomy or a lesser resection. There are no trials showing that adjuvant therapy helps reduce recurrences, but if adjuvant treatment is contemplated because of the presence of VPI, it has to be indicated regardless of the extent of resection.
However, VPI is just one of the many features associated with worse prognosis, such as cancer cells spread through air spaces (STAS), the presence of cancer cells or of their circulating DNA in the blood after resection, the presence of lymphovascular invasion or perineural permeation, and even the inadequate intraoperative lymph node assessment—the most common situation of uncertain resections—, to mention a few. These features have not been taken into account in adjuvant therapy trials, but when they have been studied, their presence worsens the prognosis of pathologic stage I lung cancers.
So, the decision to indicate adjuvant therapy should not be made just because of VPI, but other factors should be considered, too. If the decision is to administer adjuvant therapy, which seems a very intuitive decision, in the absence of clinical trials, both the patient and the physician should be aware of and agree with the limitations of the indication due to the lack of hard data supporting it.
Potential Influence on Staging Guidelines and Surgical Approaches
I don’t think the data from this trial will influence future staging guidelines. The fact that the adverse effect of VPI is independent of the type of resection does not alter the classification of the extent of the primary tumor. In addition, VPI is difficult to assess preoperatively, so it will be a finding that will appear in the final pathology report.
Regarding the surgical approach for these early-stage lung cancers, the fact that VPI worsens survival both after lobectomy and sublobar resection will not alter the indication of one or the other resection. But, as mentioned above, its presence may influence the decision to indicate adjuvant therapy with the objective to eliminate or, at least, to reduce cancer recurrence.
Important Takeaways
I think there are three important things we have learned from this trial: first, the negative prognostic impact of VPI has been confirmed even in very small tumors; second, the worse prognosis of VPI is independent of the extent of lung resection; and third, we need clinical trials to define the impact of adjuvant therapy on the prognosis of early-stage lung cancers that present with pathologic features of poor prognosis.
References
- 1. Altorki N, Wang X, Damman B, et al. Recurrence of Non–Small Cell Lung Cancer With Visceral Pleural Invasion: A Secondary Analysis of a Randomized Clinical Trial. JAMA Oncol. 2024;10(9):1179–1186. doi: 10.1001/jamaoncol.2024.2491



