








In the management of thoracic cancers, we have witnessed an exponential increase in novel treatment strategies throughout the past several years. The treatment sequence is made more challenging by the emergence and identification of resistance biomarkers, while managing severe or long-term toxicity often requires organ-specific expertise. Beyond their benefits in metastatic and recurrent lung cancer, immunotherapy and targeted therapies have also improved treatment outcomes for localized disease; and novel drugs such as antibody drug conjugates and bispecific antibodies are paving their way as potential future standards of care. While patients’ outcomes have improved, the management of their disease has become significantly more complex. In such a rapidly changing field, multidisciplinary expertise is key to optimal and successful patient care.
Multidisciplinary tumor boards (MTBs) were developed in response to important needs in patient management: to offer the most beneficial strategy at an individual level and to decrease inequity in cancer treatment across patients. An MTB’s decisions should be based on guidelines that lead to greater homogeneity, not only at the institutional level but also across institutions within a territory or region. MTBs can also address more difficult situations in which decisions must be based on expert opinions in the absence of general recommendations or clear-cut phase III data.
In France, MTBs are widely implemented in centers dedicated to cancer management. An MTB will decide upfront which guidelines are to be used—published international guidelines such as the European Society for Medical Oncology Clinical Practice Guidelines, national or regional guidelines, to which the MTB’s institution may have contributed, or local guidelines.
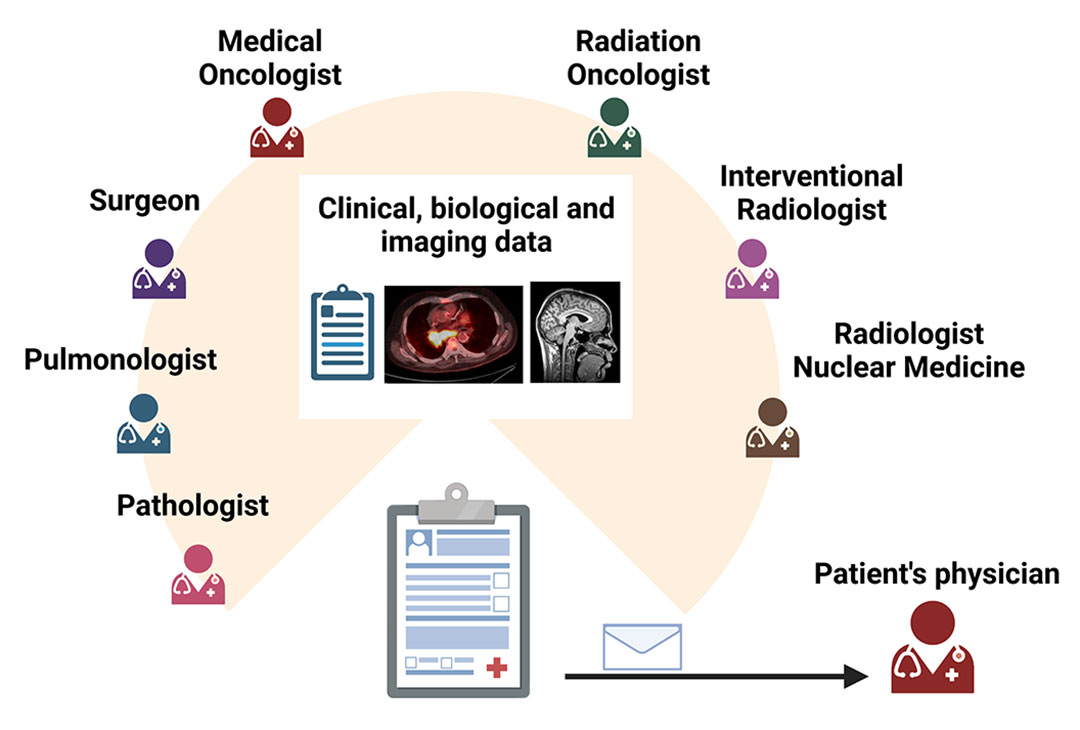
Gustave Roussy was a pathologist who created the first cancer institute in Europe in 1926. He was convinced that the multidisciplinary approach was the cornerstone of cancer management, and he created tumor boards, locally called comité. Since these first MTBs, strict standards have been maintained: the meeting should involve at least three physicians specializing in cancer management, including surgeons, medical oncologists, radiation oncologists, radiologists, interventional radiologists, pathologists, and nuclear medicine physicians (Fig. 1).
Currently, the thoracic MTB convenes once a week and discusses between 40 and 50 cases at each session. Multiple issues are addressed. Cases may be discussed for the validation of treatment proposals, such as a decision on localized treatment; or for diagnostic strategies, in those with unsampled primary or metastatic thoracic lesions. Among other questions raised in the MTB, we may discuss treatment-related toxicities, management of isolated lung lesions, or global strategies and prioritization when the patient is diagnosed with two or more synchronous cancers.
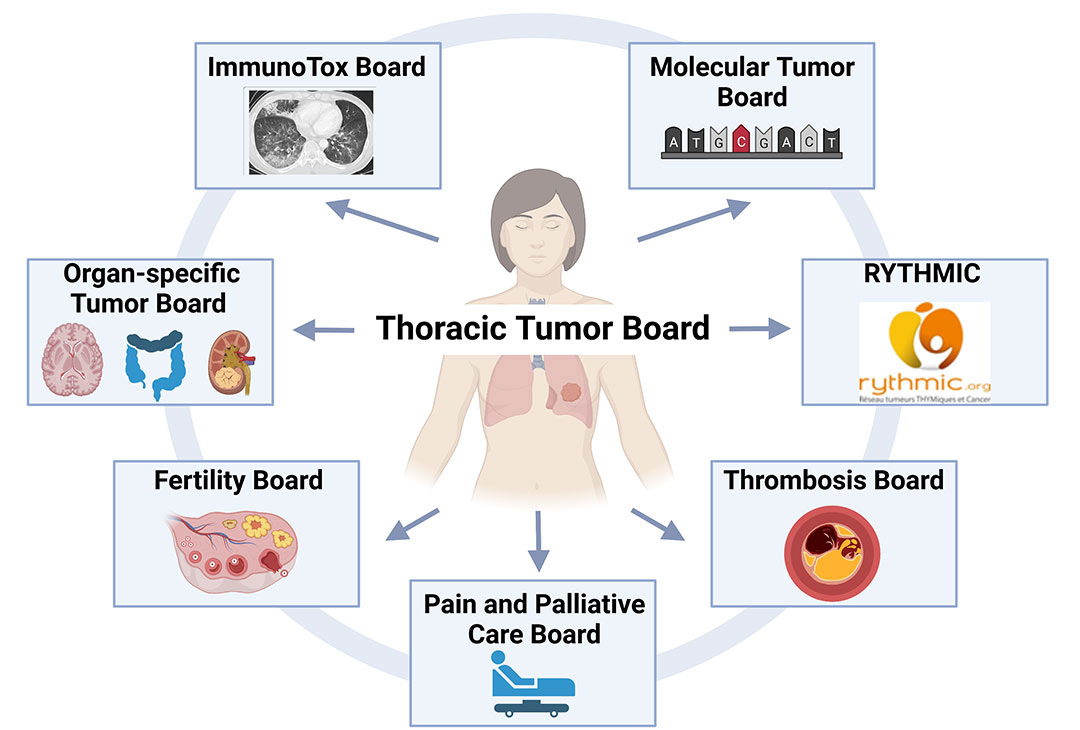
More recently, next-generation tumor boards were established at the Gustave Roussy Institute; these are highly specialized tumor boards that respond to particular needs (Fig. 2). The molecular tumor board, set up in 2010, convenes weekly and includes organ specialists, molecular biologists, and geneticists. It discusses results of next-generation sequencing for personalized treatment approaches, based on the targetability of each molecular alteration according to the ESMO Scale for Clinical Actionability of molecular Targets (ESCAT).1


The ImmunoTox Board was set up in 2016 with the aim of discussing the risk and management of immune-related adverse effects (irAEs). It takes place every 2 weeks and brings together oncologists, radiologists, pathologists, immunologists, and organ specialists. The requests addressed by this board relate to the putative causal link between immunotherapy and irAEs, the possibility of re-treatment after temporary withdrawal because of an irAE, the clinical management of complex situations, and the initiation of immunotherapy in patients with pre-existing comorbidities.2
Other MTBs that receive requests from the thoracic cancer specialists include the organ-specific tumor board, such as the neurology tumor board, called on when brain surgery is proposed for brain metastases; the thrombosis board for refractory thromboses or cases requiring invasive management; and the pain and palliative care board. Recently, a novel MTB was established—the fertility board—uniting fertility specialists, gynecologists, breast cancer specialists, oncologists, and surgeons specializing in gynecology. For lung cancer, a focus on fertility after cancer treatment is becoming more important as the number of long-term survivors increases.
At a national level, there are also MTBs dedicated to rare tumors. The tumor board RYTHMIC (Réseau Tumeurs THYmiques et Cancer) is one of 15 networks dedicated to rare malignancies set up under the umbrella of INCa (Institut National du Cancer) in the 2010s. The RYTHMIC MTB started in 2012 and was dedicated to thymomas and thymic carcinomas. Twice a month it meets to bring together national experts in rare tumors. All thymic tumor cases receive a pathology review by a national pathology panel.3 More than 3,000 cases have been discussed in almost 10 years.

Finally, the French republic includes overseas territories located on all continents and constituting 18% of all French land. Real-time, multidisciplinary videoconferencing between the French mainland and South Pacific territories was set up in 2019, and additional tumor boards were subsequently set up with other territories.4
The metrics of success for these MTBs include the reduction of human error, procurement of a panel recommendation for situations that are beyond established guidelines, and decreased waiting time for accessing specific examinations or expert opinions. One significant limitation of MTBs is the fact that decisions are based on registered data and imaging, in the absence of the central figure, the patient. Active involvement of the patient in the MTB may improve diagnostic and therapeutic decision-making and is an approach that could be tested in the era of telemedicine for selected cases with difficult decisions. Another limitation is the lack of organ-specific expertise in small hospitals, which stand to benefit from the MTBs of larger cancer centers, where such expertise exists.
Nevertheless, MTBs continue to provide a critical service with expert recommendations to assist physicians and patients in making timely and appropriate treatment decisions.
References
- 1. Mosele F, Remon J, Mateo J, et al. Recommendations for the use of next-generation sequencing (NGS) for patients with metastatic cancers: a report from the ESMO Precision Medicine Working Group. Ann Oncol. 2020;31(11):1491-1505.
- 2. Michot JM, Lappara A, Le Pavec J, et al. The 2016-2019 ImmunoTOX assessment board report of collaborative management of immune-related adverse events, an observational clinical study. Eur J Cancer. 2020;130:39-50.
- 3. Basse C, Thureau S, Bota S, et al. Multidisciplinary Tumor Board Decision Making for Postoperative Radiotherapy in Thymic Epithelial Tumors: Insights from the RYTHMIC Prospective Cohort. J Thorac Oncol. 2017;12(11):1715-1722.
- 4. Honoré C, Mir O, Geraud A, et al. Intercontinental Multidisciplinary Oncology Videoconferencing for Rare and Complex Cancer: An Alternative to Systematic Transfer. JCO Oncol Pract.



