






Tumor grading is an important component of a pathology report, as it has been traditionally used as a prognostic indicator. For many tumors, grading is also used to help with case management and patient treatment, such as for breast, prostate, and urothelial carcinomas. Grading is based on a pattern or patterns of tumor growth (the degree of differentiation in tubular formation) in association with nuclear and cytology features and mitotic counts.
Pulmonary adenocarcinomas are histologically heterogeneous and present with multiple combinations of patterns and proportions. The current classification of invasive pulmonary adenocarcinoma that is based on the predominant histologic pattern suggests a good correlation with prognosis. It has been well demonstrated that a stage 1 lepidic (predominant) adenocarcinoma has a low risk of recurrence, in contrast to a solid or micropapillary predominant tumor that has a higher recurrence rate1
,2
. However, the classification cannot be used for histologic grading because it does not address the heterogeneity of patterns seen in pulmonary adenocarcinoma. For example: How should a lepidic predominant tumor with a solid component be graded? Can we assume that the solid component won’t drive a risk of recurrence? What other features may affect tumor behavior and prognosis?
Several studies have suggested that other histologic patterns within the tumor, as well as additional features such as nuclear grade,3
mitotic counts,4
and the presence of spread through air spaces (STAS),5
can influence prognosis. However, there has been no systematic approach to evaluating and incorporating those features into a grading system.
The IASLC Pathology Committee has addressed these issues and proposed a new grading system for pulmonary adenocarcinoma in a recent publication in the Journal of Thoracic Oncology.6
The study was conducted using several well-annotated, independent data sets from multiple institutions, thus reducing institution and pathologist biases.
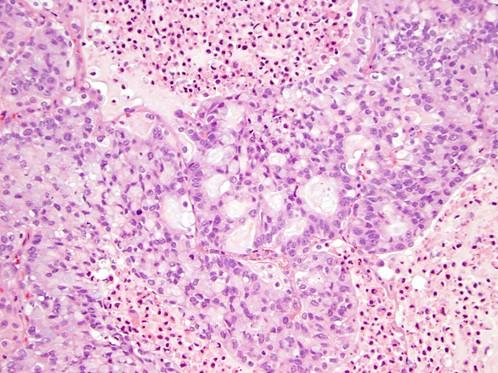
One data set consisting of 284 cases of stage I adenocarcinoma was used as a discovery and training cohort in which multiple parameters were tested. Because predominant pattern has been shown to have a strong association with prognosis, it was used as the basis of the model. Predominant pattern plus several combinations of other patterns were also tested, and the combination of the predominant plus highest-grade pattern in the tumor was considered the best model. High grade pattern included complex glandular patterns and cribriform pattern (Fig. 1), as originally proposed by Sica and colleagues,7
along with solid and micropapillary patterns, whereas conventional acinar and papillary patterns were classified as intermediate grade and lepidic were classified as low grade.
Fig. 1. Complex Glandular Pattern (Cribriform) Has Been Recognized as a High-Grade Histologic Pattern
Other histologic features such as nuclear grade, mitotic counts, cytologic atypia, and the presence of STAS did not contribute to a prognostic performance of the model, although all of these features were individually associated with prognosis. It has also become clear that these features are associated with histologic growth patterns. For example, high nuclear grade, mitotic counts, cytologic atypia, and STAS are more commonly seen in solid/complex glandular patterns, even if the latter are not the predominant patterns in the tumor. The only exception is micropapillary pattern, which is associated with low nuclear grade, cytologic atypia, and mitotic counts, although it has been known to associate with a high risk of recurrence and the presence of STAS.
Because the grading system was to be based solely on a pattern or patterns of growth, it became imperative to determine the minimal amount of any high-grade pattern (all high-grade patterns seen in the tumor collectively) that would have an effect on prognosis. It was determined that a cutoff of 20% of high-grade patterns would offer the best combination of sensitivity and specificity of the model predicting prognosis. Thus, we have implemented the 20% cutoff in the model and proposed a new grading system—the IASLC grading system—for pulmonary adenocarcinoma, as summarized in the Table. In accordance with the system, a tumor that is composed predominantly of acinar pattern (60%) with 30% lepidic and 10% micropapillary patterns is graded as moderately differentiated (grade 2), whereas a tumor with 50% acinar, 20% lepidic, and 30% solid patterns is graded as poorly differentiated (grade 3).
Table. Grading for Invasive Adenocarcinomas
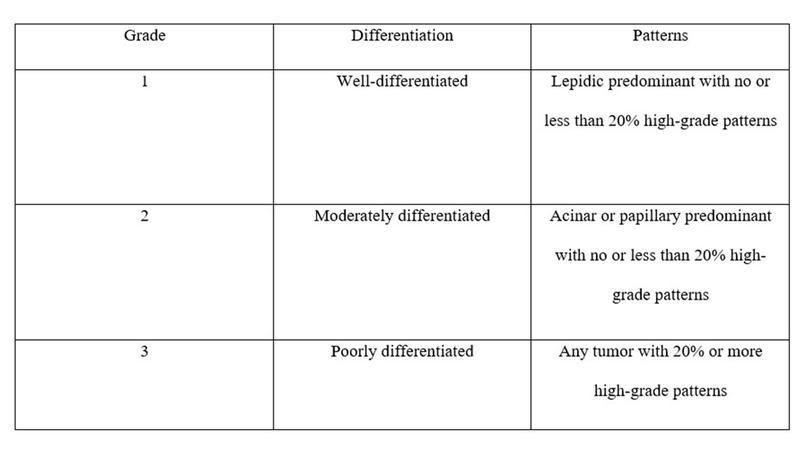
Reproduced with permission from Moreira AL, Ocampo PSS, Xia Y. A grading system for invasive pulmonary adenocarcinoma: a proposal from the International Association for the Study of Lung Cancer Pathology Committee. J Thorac Oncol. 2020;15(10):1599-1610.
The same parameters used for the creation of the grading system in the training and discovery cohort were applied to a cohort of 212 cases of stage I adenocarcinoma (a validation set). Similar to the training cohort, the combination of the predominant plus high-grade patterns was the best indicator of recurrence. Again, addition of any other histologic features did not improve the prognostic performance of the model.
Finally, the model was tested in another cohort composed of stage I to III cases of adenocarcinoma, with similar results. Kaplan–Meier curves showed that the stratification of recurrence-free survival between the three grades in the entire cohort, as well as for stage I tumors, was more evident with the IASLC grading system compared to that with the predominant-pattern–based classification (see Fig. 2). The reproducibility of the model was also tested, and there was substantial agreement among observers using Fleiss κ test and almost perfect agreement between pairs of the observers.
Fig 2. Kaplan-Meier Curves for Recurrence-Free Survival of the Test Cohort, Stratified by Grading System
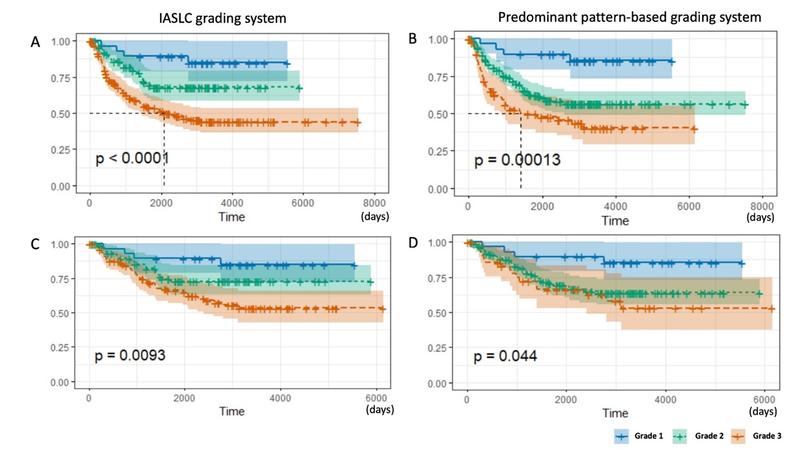
IASLC grading system: A—the entire cohort; C—stage I cohort. Predominant-pattern–based grading system: B—the entire cohort; D—stage I cohort.
Reproduced with permission from Moreira AL, Ocampo PSS, Xia Y. A grading system for invasive pulmonary adenocarcinoma: a proposal from the International Association for the Study of Lung Cancer Pathology Committee. J Thorac Oncol. 2020;15(10):1599-1610.
The article from the IASLC Pathology Committee demonstrates that a grading system based on histologic pattern is a strong prognostic classifier of invasive pulmonary adenocarcinoma. It is practical and easy to apply; it does not require further training for pathologists, as it has been built directly on the current pattern-based classification system. The model is reproducible in multiple data sets from multiple institutions. We hope this grading system will be used as a common language in clinical practice, and especially by investigators in clinical trials and other studies evaluating prognostic and/or predictive markers in pulmonary adenocarcinoma, thus allowing for more comprehensive comparison of the histologically heterogeneous tumors.
- 1. Yoshizawa A, Motoi N, Riely GJ, et al. Impact of proposed IASLC/ATS/ERS classification of lung adenocarcinoma: prognostic subgroups and implications for further revision of staging based on analysis of 514 stage I cases. Mod Pathol. 2011;24(5):653-664.
- 2. Warth A, Muley T, Meister M, et al. The novel histologic International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society classification system of lung adenocarcinoma is a stage-independent predictor of survival. J Clin Oncol. 2012;30(13):1438-1446.
- 3. Nakazato Y, Minami Y, Kobayashi H, et al. Nuclear grading of primary pulmonary adenocarcinomas: correlation between nuclear size and prognosis. Cancer. 2010;116(8):2011-2019.
- 4. von der Thüsen JH, Tham YS, Pattenden H, et al. Prognostic significance of predominant histologic pattern and nuclear grade in resected adenocarcinoma of the lung: potential parameters for a grading system. J Thorac Oncol. 2013;8(1):37-44.
- 5. Kadota K, Nitadori JI, Sima CS, et al. Tumor Spread through Air Spaces is an Important Pattern of Invasion and Impacts the Frequency and Location of Recurrences after Limited Resection for Small Stage I Lung Adenocarcinomas. J Thorac Oncol. 2015;10(5):806-814.
- 6. Moreira AL, Ocampo PSS, Xia Y. A grading system for invasive pulmonary adenocarcinoma: a proposal from the International Association for the Study of Lung Cancer Pathology Committee. J Thorac Oncol. 2020;15(10):1599-1610.
- 7. Sica G, Yoshizawa A, Sima CS. A grading system of lung adenocarcinomas based on histologic pattern is predictive of disease recurrence in stage I tumors. Am J Surg Pathol. 2010;34(8):1155-1162.



